Spike in colorectal cancer rates among younger Americans
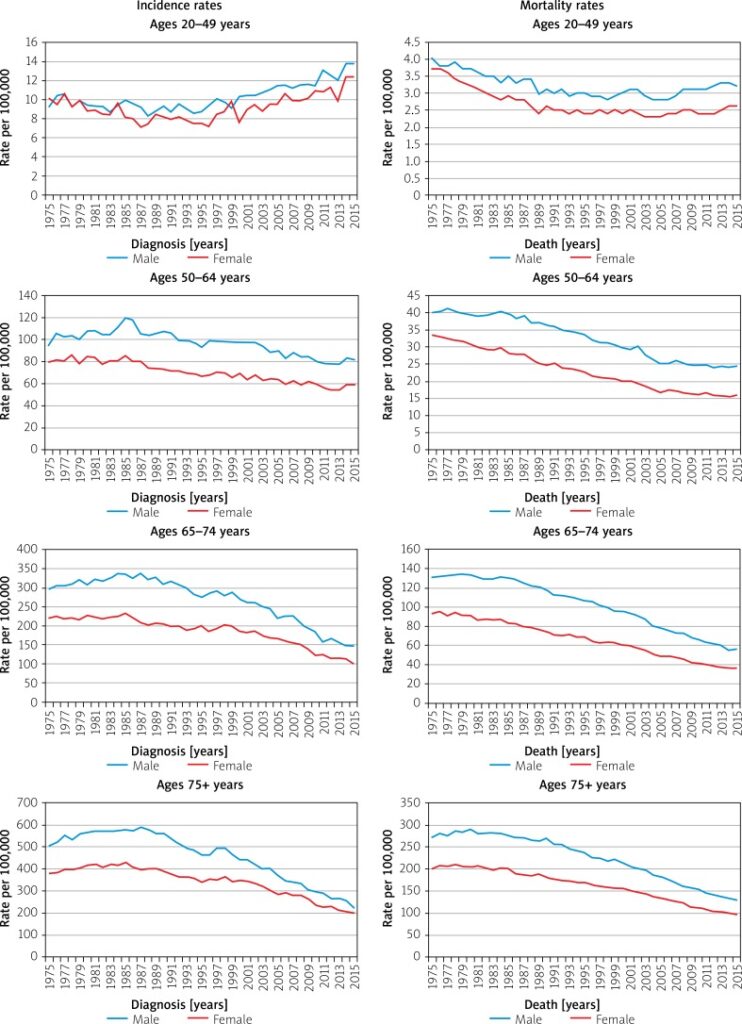
Not due to earlier detection and diagnoses -> mortality rates are rising from previous decades
“This is not merely a phenomenon of picking up more small cancers… There is something else going on that’s truly important.”
Dr. Thomas Weber, https://www.nytimes.com/2017/08/22/well/live/more-young-people-are-dying-of-colon-cancer.html
Researchers are not exactly sure why, but there are speculations:
There is a study that found prolonged antibiotics use in adulthood to be associated with greater risk for precancerous polyps -> antibiotics alter gut bacteria
Younger people have polyps that are harder to see and remove during colonoscopies
Policy changes?
Expanding universal screening -> more controversial and costly -> question: are we making young people go thru screening for no reason?
Frequent complications from. colonoscopies -> other testing options encouraged
Concerns over false positives and negatives
Reflections/questions:
The statistics and findings of the new study reflect higher death rates rather than just earlier detection and diagnosis, which challenge the common, long-held myth that cancer is a disease of the old, which is explored often in our class readings, specifically Jain’s book.
In the context of screening and detection, the article raises the importance of screening for younger generations and new risk factors previously unknown to the common population.
How can we examine the issue of earlier screening and factor in young people’s increasing burden of cancer?
What does it mean when the risk of developing colon cancer is associated with a ‘Western’ diet and lifestyle?
‘Western’ diet -> defined as high in red meats, fatty products, refined grains and desserts
The study found that those who closely follow this diet were more than 3x likely to relapse than those whose diets were at the opposite end of the scale
Authors stress that this study is observational and does not provide conclusive proof
“… people treated for locally advanced colon cancer can actively improve their odds of survival by their dietary choices”
Jeffrey Meyerhardt
When Googling ‘Western diet’, this is what I found on the image tab.
“Maybe the message is it’s never too late to change your diet”
Andrejs Avots- Avotins
Reflections/questions:
What does this mean in context of socioeconomic status and other factors? Is it always feasible to change diet and improve outcomes/avoid cancer risks? How does diet interact with other factors?
Emphasis on individual lifestyle choices rather than broader contexts
Would this place blame on individuals rather than systems? (specifically, blaming individuals in the study who ascribe to the Western diets)
Taken out of context, this study could’ve been shown to others with the basis that diet is a very big factor that causes cancer rather than is associated with it (and still needs more research)
Boyer’s reflections in The Undying: The media, research, the Internet, and seemingly everything is telling cancer patients to try different things and to attribute survival on select few factors dependent on choice rather than to look at cancer more broadly at a societal level
“The first words that came out of my mouth were, ‘But I ‘m only 27.’ I couldn’t say much because I was in shock.”
Betancourt, upon hearing her diagnosis. https://www.self.com/story/young-women-living-with-colon-cancer
Rates of colorectal cancers are increasing among millennials
Both Rosen and Betancourt needed to have treatment right away and have surgery to remove the tumor (or in Rosen’s case, her entire colon had to be removed as she has Crohn’s disease which means her colon is at risk of developing cancer again)
Side effects and changes from treatments and cancer:
Betancourt: Ileostomy and losing hair as side effects made her feel like she was losing her identity and worth
Betancourt also needed a hip replacement after a chemo drug damaged her hip
Rosen: treatments impacted her fertility and a routine colonoscopy caused her to have to remove her rectum and anus
Important to have young patient voices and advocacy to dispel the myth that cancer is an ‘old people disease’
Jain also discussed this in Malignant: Lack of patient education is a big problem that affects young adult survival
Illuminating side effects and changes due to cancer that is not often spoken about, especially for a cancer like colon cancer where people don’t want to speak about (or hear about) bowel movements or organs related to them
Permanently disfiguring for both Rosen and Betancourt
Colorectal cancer (or CRC) is the third most deadly & fourth most commonly diagnosed cancer in the world
CRC incidence rising worldwide -> in developing countries with more ‘Western’ diets
In countries undergoing many developments -> higher incidences with increasing human development index (HDI)
Does this take into account completeness and effectiveness of cancer registries/databases, screening, and behaviors such as reporting?
Map with age-standardized incidences in 2018 across both sexes and ages.
Risk factors/behaviors
Obesity
Diabetes
Family history/hereditary disorders
Inflammatory bowel diseases
Ulcerative colitis + Crohn’s disease -> affect people with lower income and educational status the worst
Sedentary lifestyle
Red/processed meat consumption
Alcohol, tobacco
Reducing CRC mortality -> early detection screenings, treatment options, genetic testing, family history documentation
More incidence among men than women
(Why?)
Adults aged 20-49 (out of usual age ranges for screening) -> growing incidence
Dispel the myth that cancer is an ‘old people’ disease
Is this age-related incidence rising only happening to CRC or to other cancers as well?How are we documenting this?
Survival
Decreases in mortality could be due to early detection screenings and efforts (removal of polyps, colonoscopies, blood testing)
Five year survival rate depending on stages
Stage 1: 92%
Stage IIA: 87%, stage IIB: 65%
Stage IIIA: 90%, stage IIIB: 72%, stage IIIC: 53%
Stage IV (metastatic): 12%
Why are rates for stage IIIA and IIIB higher than the stage II?
Survival varies depending on race and status
Up to 30% of CRC patients have family history of neoplasm
Lynch syndrome and other hereditary risk factors -> genetic diagnosis are too costly -> family history remains in data-taking -> will this be effective in populations w/o access to care and consistent history-taking? (i.e rural populations lacking specialists/ PCP)
More on Race
-> Observation: racial identification/categorization in the above graph is unclear and confusing. This resonates with How Cancer Crossed the Color Line and its analysis of inconsistent demographic and racial categories in databases which influence statistics. In what way do numbers and statistics of cancer influence ontology? Historically race categorization has been fluid depending on the social views accepted at the time -> what are some other ways to report demographical data better?
African Americans and Native Americans have higher incidences of CRC and lower survival among all CRC stages
Use certain medications (NSAIDSs) have protective effects against CRC
Reflections/questions:
Necessity of numbers in epidemiological studies -> yet, are cancer patients suffering ‘violence by abstraction’? (Jain, Malignant)
The Mortality Effect: immortal logic of science + data vs. individual mortality
Statistical logic and its dangers
Prognostic stats are at once transparent and confusing… it means everything and nothing at once, especially regarding survival
Ontology of cancer through numbers and trends: We derive our treatment and knowledge off of data, but how much is this data hidden/skewed, and how does that affect the way we understand and perceive cancer?
Fluid and ever-changing categorization of race as an example
Ethnography in Indonesia -> Community-based risk reduction
Low + middle income countries have rising incidence of colorectal cancer (aging population + sedentary lifestyle, westernized behavior lifestyle)
Does westernized behavior necessarily correlate with cancer? And how so? (dangers of the simplified model of civilization = cancer and primitivism = safe from cancer -> How Color Crossed the Cancer Line book)
Cultural influences on health beliefs/values/behaviors
CRC screening less supported in Asia (equipments + specialists costs)
Data collected from observation, interviews, focus group discussions, thematic analysis
Themes:
Food preparation (cook freshly rather than refrigerate)
Food cooking (low sodium salt and limit flavor additives)