The data aggregation problem and health disparities
Third most common cancer in the U.S
Asian American subgroups vary widely -> problem of data registries and research aggregating them into one group
Discussed by Wailoo’s book How Cancer Crossed the Color Line -> historically race and ethnicity has been defined arbitrarily by the dominant group (white) -> all other groups are aggregated in terms because they are ‘other’ to the white group, therefore being blind to each group’s own internal diversity
Heterogeneity in incidence -> related to country of origin, diet, screening, and lifestyle choices
Japanese Americans have the highest incidence, and all incidence are increasing among other groups except for Korean Americans
CRC incidence is highest among non-Hispanic black populations, lowest among Asians/Pacific Islanders
SEER program only started collecting data on Hispanic Americans and Asians/Pacific Islanders since 1990
What does this say about missing data and inability to create historical trends?
Gap between mortality rates among Black and White Americans have increased over the last 3 decades
Disparities exist between races but also within
Screening prevalence lower among ages younger than 65, non-White, less educated, without insurance, recent immigrants, Hispanic people, and those with language barriers
Asians are less likely to screen than non-Hispanic whites
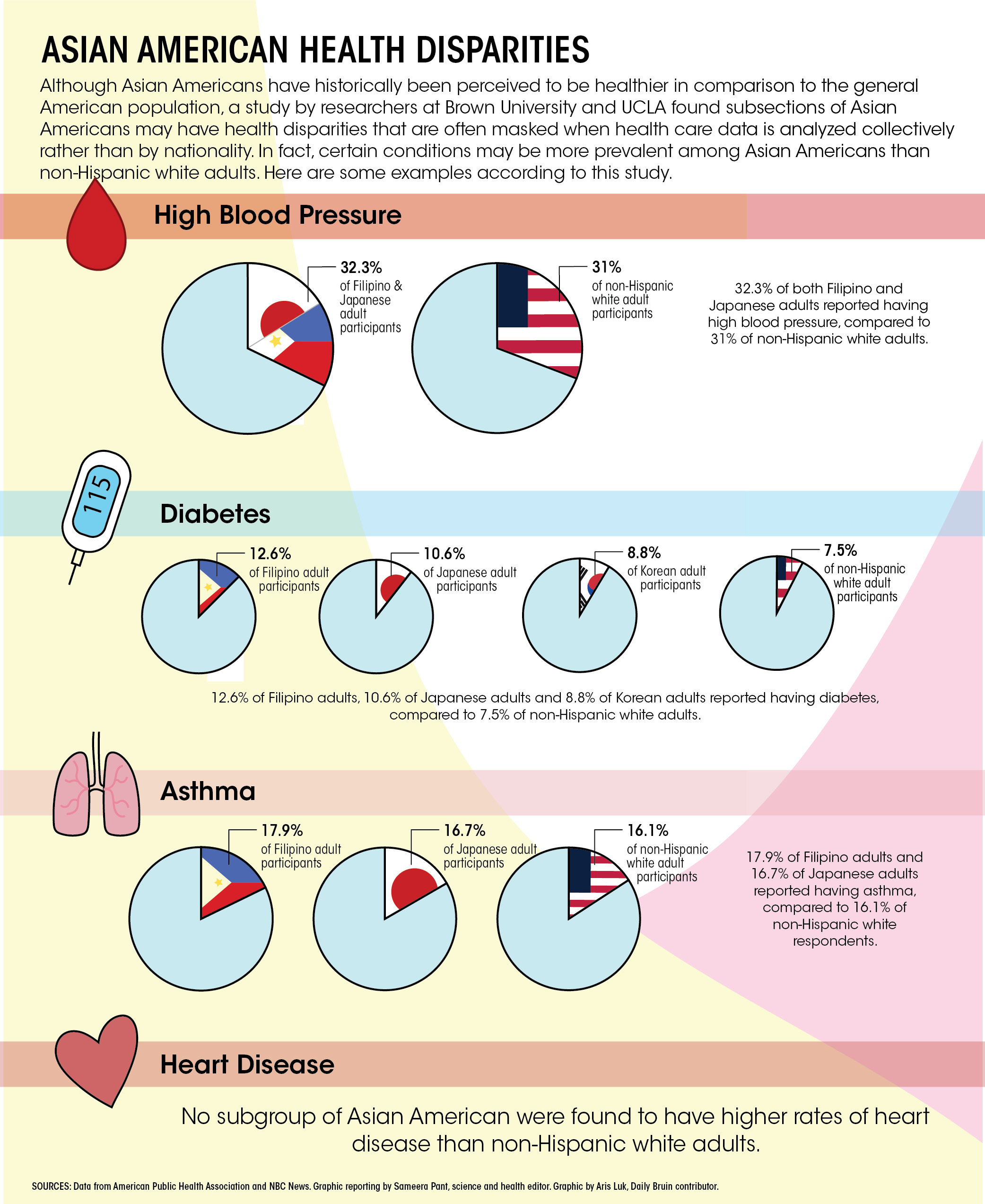
A study finding that data aggregation of Asian American subgroups conceal health risks. Article found from here: https://dailybruin.com/2020/03/06/study-shows-aggregated-data-conceals-asian-american-subgroup-health-problems
A study found “the Western diet increases colon cancer by deregulating bile acid homeostasis, and activating colon cell proliferation”
Dietary chemoprevention -> cultural aspects of diet and lifestyle in Asian Americans in cancer prevention
unpolished Thai rice and reduced CRC risk because of high phytochemical contents
Sea cucumbers, abalones are both Asian delicacies are shown to have anti-tumor properties
Risk factor: Risk increases among Asian Americans as their diet becomes ‘Westernized’
Asians with longer immigration history parallel cancer risk patterns of U.S natives
Asians with more recent immigration history parallel cancer risk patterns of home countries
Reflections/questions
Emphasizes the need for more complete data (Flaws in databases and data collection methods: Primarily in English, did not capture populations with low English proficiency, vary in time frame/sample size/geography, SEER data is more recent on Asians)
Perhaps more data on cultural and behavioral factors that influence prevention and screening?
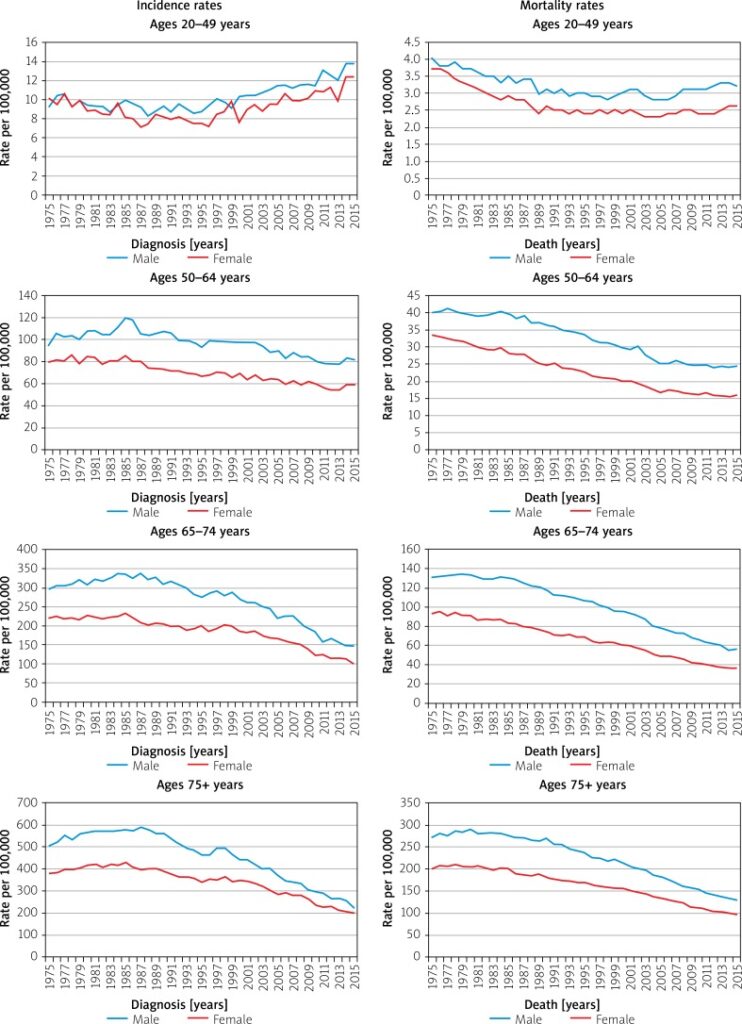
Spike in colorectal cancer rates among younger Americans
Not due to earlier detection and diagnoses -> mortality rates are rising from previous decades
“This is not merely a phenomenon of picking up more small cancers… There is something else going on that’s truly important.”
Dr. Thomas Weber, https://www.nytimes.com/2017/08/22/well/live/more-young-people-are-dying-of-colon-cancer.html
Researchers are not exactly sure why, but there are speculations:
There is a study that found prolonged antibiotics use in adulthood to be associated with greater risk for precancerous polyps -> antibiotics alter gut bacteria
Younger people have polyps that are harder to see and remove during colonoscopies
Policy changes?
Expanding universal screening -> more controversial and costly -> question: are we making young people go thru screening for no reason?
Frequent complications from. colonoscopies -> other testing options encouraged
Concerns over false positives and negatives
Reflections/questions:
The statistics and findings of the new study reflect higher death rates rather than just earlier detection and diagnosis, which challenge the common, long-held myth that cancer is a disease of the old, which is explored often in our class readings, specifically Jain’s book.
In the context of screening and detection, the article raises the importance of screening for younger generations and new risk factors previously unknown to the common population.
How can we examine the issue of earlier screening and factor in young people’s increasing burden of cancer?
Colorectal cancer (or CRC) is the third most deadly & fourth most commonly diagnosed cancer in the world
CRC incidence rising worldwide -> in developing countries with more ‘Western’ diets
In countries undergoing many developments -> higher incidences with increasing human development index (HDI)
Does this take into account completeness and effectiveness of cancer registries/databases, screening, and behaviors such as reporting?
Map with age-standardized incidences in 2018 across both sexes and ages.
Risk factors/behaviors
Obesity
Diabetes
Family history/hereditary disorders
Inflammatory bowel diseases
Ulcerative colitis + Crohn’s disease -> affect people with lower income and educational status the worst
Sedentary lifestyle
Red/processed meat consumption
Alcohol, tobacco
Reducing CRC mortality -> early detection screenings, treatment options, genetic testing, family history documentation
More incidence among men than women
(Why?)
Adults aged 20-49 (out of usual age ranges for screening) -> growing incidence
Dispel the myth that cancer is an ‘old people’ disease
Is this age-related incidence rising only happening to CRC or to other cancers as well?How are we documenting this?
Survival
Decreases in mortality could be due to early detection screenings and efforts (removal of polyps, colonoscopies, blood testing)
Five year survival rate depending on stages
Stage 1: 92%
Stage IIA: 87%, stage IIB: 65%
Stage IIIA: 90%, stage IIIB: 72%, stage IIIC: 53%
Stage IV (metastatic): 12%
Why are rates for stage IIIA and IIIB higher than the stage II?
Survival varies depending on race and status
Up to 30% of CRC patients have family history of neoplasm
Lynch syndrome and other hereditary risk factors -> genetic diagnosis are too costly -> family history remains in data-taking -> will this be effective in populations w/o access to care and consistent history-taking? (i.e rural populations lacking specialists/ PCP)
More on Race
-> Observation: racial identification/categorization in the above graph is unclear and confusing. This resonates with How Cancer Crossed the Color Line and its analysis of inconsistent demographic and racial categories in databases which influence statistics. In what way do numbers and statistics of cancer influence ontology? Historically race categorization has been fluid depending on the social views accepted at the time -> what are some other ways to report demographical data better?
African Americans and Native Americans have higher incidences of CRC and lower survival among all CRC stages
Use certain medications (NSAIDSs) have protective effects against CRC
Reflections/questions:
Necessity of numbers in epidemiological studies -> yet, are cancer patients suffering ‘violence by abstraction’? (Jain, Malignant)
The Mortality Effect: immortal logic of science + data vs. individual mortality
Statistical logic and its dangers
Prognostic stats are at once transparent and confusing… it means everything and nothing at once, especially regarding survival
Ontology of cancer through numbers and trends: We derive our treatment and knowledge off of data, but how much is this data hidden/skewed, and how does that affect the way we understand and perceive cancer?
Fluid and ever-changing categorization of race as an example