- Silence -> seen as ‘not getting upset in front of each other’ -> preserves relationships in CRC oncology clinic
- Silence as relational form of moral work that preserves others’ well-being
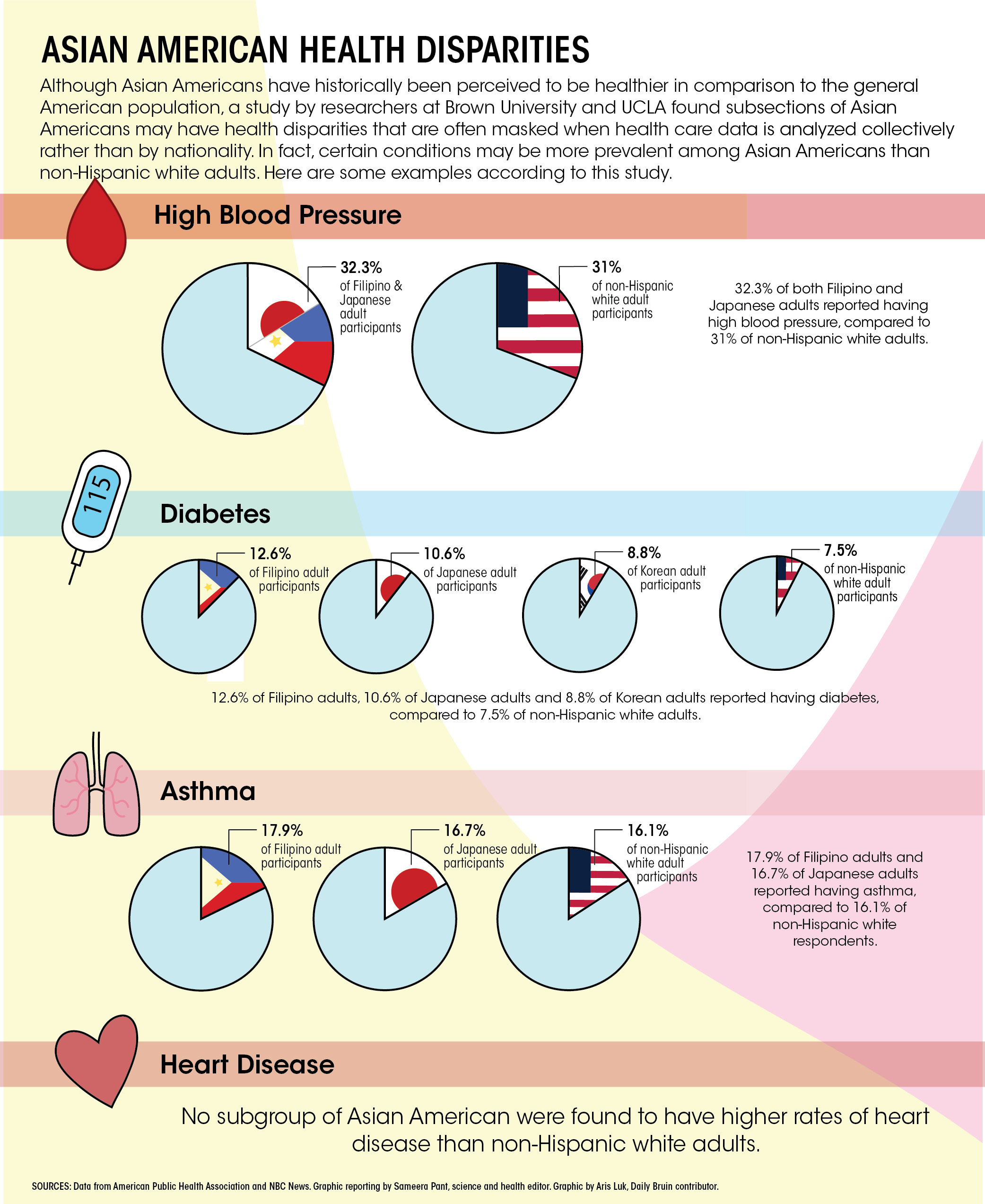
- Studies show a lot of emotional distress among patients with and beyond CRC
- 1/5 people affected by CRC has a post-cancer diagnosis of depression
- Emotion work in surface acting vs. deep acting
- Embodied emotional experiences and the performative role of emotions
- The study follows participants through treatment pathway until there was no evidence of disease in their bodies or referred to hospices
- Some focus on pragmatism/practicality rather than emotions
- Many manage expressions of emotions continuously in front of others
- Nurses are cognizant of emotional texture of cancer treatments
“We just try to open it up and give them an opportunity to talk about [what they are feeling]. It is often letting them be cross, or to be angry, or to be frustrated, because all are logical and normal emotions to have during cancer treatments”
A Filipina senior chemotherapy nurse.
- Staff and health professionals also have to do some emotional labor -> keeping boundaries and maintaining balance between distance and closeness to patients while keeping their emotional peace
- Nurses are expected to connect with patients to do emotional labor in contrast to physicians, many of whom decided to pursue a ‘happier’ field
- Many patients in the CRC support group disclosed the need to do emotion work as to not ‘burden others’ in fear of damaging relationships with others
- The relatives also experience this fear of being a burden
- Existing norms surrounding emotional management of relatives -> to not be upset because expressing it would impact their loved ones
Silence: reconsidered as relational practice of moral work, not maladaptive coping behavior
- Reflections/questions:
- Silence as moral relational work connects to