“The first words that came out of my mouth were, ‘But I ‘m only 27.’ I couldn’t say much because I was in shock.”
Betancourt, upon hearing her diagnosis. https://www.self.com/story/young-women-living-with-colon-cancer
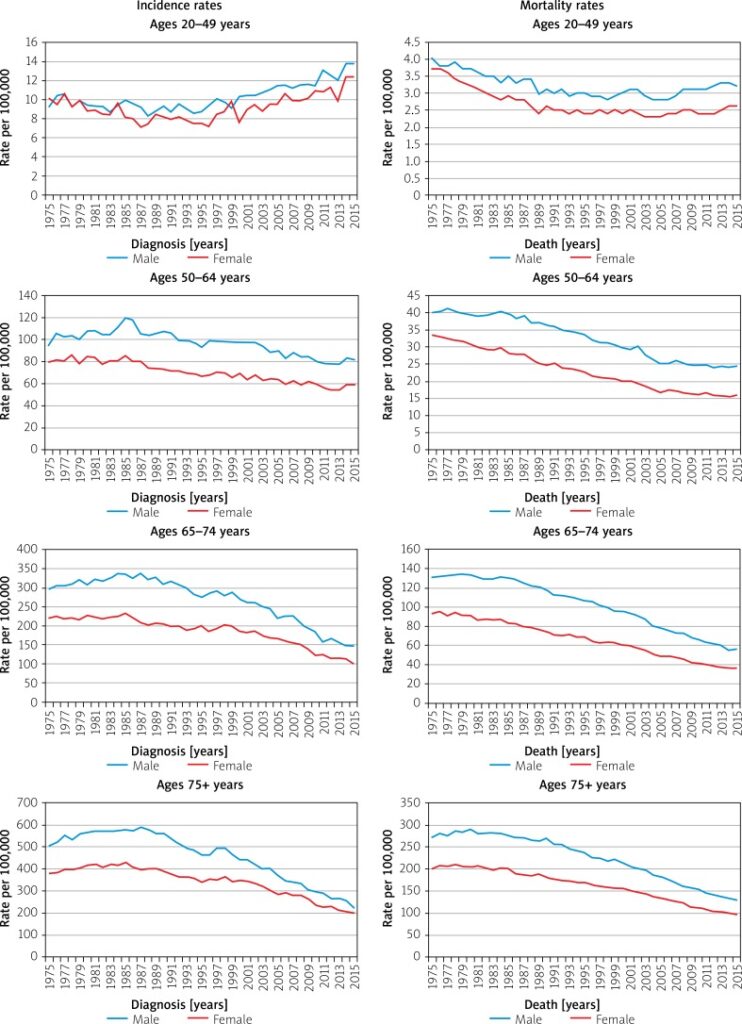
Rates of colorectal cancers are increasing among millennials
Both Rosen and Betancourt needed to have treatment right away and have surgery to remove the tumor (or in Rosen’s case, her entire colon had to be removed as she has Crohn’s disease which means her colon is at risk of developing cancer again)
Side effects and changes from treatments and cancer:
Betancourt: Ileostomy and losing hair as side effects made her feel like she was losing her identity and worth
Betancourt also needed a hip replacement after a chemo drug damaged her hip
Rosen: treatments impacted her fertility and a routine colonoscopy caused her to have to remove her rectum and anus
Important to have young patient voices and advocacy to dispel the myth that cancer is an ‘old people disease’
Jain also discussed this in Malignant: Lack of patient education is a big problem that affects young adult survival
Illuminating side effects and changes due to cancer that is not often spoken about, especially for a cancer like colon cancer where people don’t want to speak about (or hear about) bowel movements or organs related to them
Permanently disfiguring for both Rosen and Betancourt
Phil Scamihorn’s story, also recounted in his blog
Decision to get a blog -> To keep others informed of progress and gain a community supporting him
Community as crucial
He offers support to newly diagnosed patients
Online support community Cancer Survivors Network
Scamihorn did his own research and got second opinion from other oncologists
The oncologist team that he went with won his confidence/trust
Hope, trust and common goal-setting as an important factor in patient-doctor relationships (“Most important, the doctor told him that stage 4 colon cancer can be cured”)
Scamihorn was diagnosed at 47 so his children would be screened 10 years earlier
“There are many patients in the online support community who have had five years without cancer,” says Scamihorn, now 53. “I also encourage people to find a doctor they trust, someone they’re comfortable with, and let them do their job.”
His decision to get a blog -> connects to this resource discussing importance of cancer patients writing/creating media as outlet and to shape identity through experience -> authentic patient voices help dispel illness myths and deepen understanding
Trust and communication as crucial -> Scamihorn felt more trust and confident working with his second opinion
How can doctors better use this understanding to inform their practices?
Colorectal cancer (or CRC) is the third most deadly & fourth most commonly diagnosed cancer in the world
CRC incidence rising worldwide -> in developing countries with more ‘Western’ diets
In countries undergoing many developments -> higher incidences with increasing human development index (HDI)
Does this take into account completeness and effectiveness of cancer registries/databases, screening, and behaviors such as reporting?
Map with age-standardized incidences in 2018 across both sexes and ages.
Risk factors/behaviors
Obesity
Diabetes
Family history/hereditary disorders
Inflammatory bowel diseases
Ulcerative colitis + Crohn’s disease -> affect people with lower income and educational status the worst
Sedentary lifestyle
Red/processed meat consumption
Alcohol, tobacco
Reducing CRC mortality -> early detection screenings, treatment options, genetic testing, family history documentation
More incidence among men than women
(Why?)
Adults aged 20-49 (out of usual age ranges for screening) -> growing incidence
Dispel the myth that cancer is an ‘old people’ disease
Is this age-related incidence rising only happening to CRC or to other cancers as well?How are we documenting this?
Survival
Decreases in mortality could be due to early detection screenings and efforts (removal of polyps, colonoscopies, blood testing)
Five year survival rate depending on stages
Stage 1: 92%
Stage IIA: 87%, stage IIB: 65%
Stage IIIA: 90%, stage IIIB: 72%, stage IIIC: 53%
Stage IV (metastatic): 12%
Why are rates for stage IIIA and IIIB higher than the stage II?
Survival varies depending on race and status
Up to 30% of CRC patients have family history of neoplasm
Lynch syndrome and other hereditary risk factors -> genetic diagnosis are too costly -> family history remains in data-taking -> will this be effective in populations w/o access to care and consistent history-taking? (i.e rural populations lacking specialists/ PCP)
More on Race
-> Observation: racial identification/categorization in the above graph is unclear and confusing. This resonates with How Cancer Crossed the Color Line and its analysis of inconsistent demographic and racial categories in databases which influence statistics. In what way do numbers and statistics of cancer influence ontology? Historically race categorization has been fluid depending on the social views accepted at the time -> what are some other ways to report demographical data better?
African Americans and Native Americans have higher incidences of CRC and lower survival among all CRC stages
Use certain medications (NSAIDSs) have protective effects against CRC
Reflections/questions:
Necessity of numbers in epidemiological studies -> yet, are cancer patients suffering ‘violence by abstraction’? (Jain, Malignant)
The Mortality Effect: immortal logic of science + data vs. individual mortality
Statistical logic and its dangers
Prognostic stats are at once transparent and confusing… it means everything and nothing at once, especially regarding survival
Ontology of cancer through numbers and trends: We derive our treatment and knowledge off of data, but how much is this data hidden/skewed, and how does that affect the way we understand and perceive cancer?
Fluid and ever-changing categorization of race as an example
Colorectal cancer (CRC) links to accumulation of genetic and epigenetic changes to the genome
Accumulated through chromosomal instability, micro satellite instability, CpG island methylator phenotype.
Formation of inflammatory milieu -> tumor development/progression
Dendritic cells impairments
Not recruiting enough activated effector T cells
Creation of dominant immune inhibitory mechanisms that usurp T cell effector functions
Potential biomarkers for checkpt blockade therapy
Biomarkers for therapy would be very helpful in translational research and to evaluate effectiveness of therapy
Changes in tumor microenvironment resembles chronic inflammation
Dendritic cells as candidates in cancer vaccines of CRC patients -> generate more host immune responses against tumor antigens
Challenges: they might lose activity in cancer environment + Interactions with T cell regulators (Treg) actually enhance immunosuppression
Is there a way to fully activate dendritic cells (selectively with adjuvants) while keeping Treg from expansion and function?
Reflection/questions:
Importance of understanding mechanisms behind cancer interactions and immune system -> can reverse dendritic cell as immunosuppressive in cancer to immunostimulatory
Will dendritic cell-based therapy be more effectiveness in patients with a specific type of CRC?
Cytokines = proteins which play important role in cell signaling (IL-17 cytokines promote inflammation -> drive tumor growth on colon -> colon cancer)
Professor Wang discovered removing IL-17 signaling on regulatory T cells (Tregs) increase colon tumor development
Tregs = often recruited to tumors, hinder body’s ability to impede tumor growth
IL-17 has site specific inhibition
Colon tumor under fluorescent microscopy.
This means IL-17 inhibits Tregs that would otherwise suppress cancer immunosurveillance while also inhibiting the attraction of T cells that would perform this function. These findings illuminate the complicated role of IL-17 in colorectal cancer and showcase the need for further investigation.
More research should be done on dendritic cells’ immune functions
Unless there already are some?
New therapies for resistant colorectal cancer -> clinical trial using immune checkpoint inhibitor + dendritic growth factor Flt3L
When the team augmented the number of dendritic cells within liver metastases…. the treatment led to an increase in cytotoxic T lymphocytes within the tumors and caused the tumors to become sensitive to immune checkpoint inhibitors.
Chaos narrative (anti-narrative, time without sequence, reflection but non-reflection)
Perhaps this is more of Anne Boyer’s approach in her The Undyingbook
Patients not only restore the experiential dimension
to illness and treatment, but also place the ill person
at the very centre of that experience.
Anne Hunsaker Hawkins (1999)
Cancer diagnosis as de-stabilizing/ de-humanizing, invasive
Importance of narratives to counter self- fragmentation -> producing identity and experience as the patient is experiencing it.
Reflections:
Illness portrayals (commonly seen in mental illness)-> inaccurate in media/ inauthentic -> reading these accounts create incongruence-> stereotypes and myths do not aid interactions between others and the patient -> stigma
Important questions:
“Does this text voice illness, fictional or not, in a way that creates agency and empowerment for the reader or does it advance the cliché that proximity to death creates profundity?”
“Does the voice actually advance an understanding of illness or simply present an emotional melodrama?”
Jarring contrast between lived experiences of youths with cancer vs. the story -> perpetuate illness myths -> usurping of patient voice
“I do not exist to be your tragedy. I do not exist for you to find special meaning in your life. I do not exist to teach people lessons or to give people feels.”
Ethnography in Indonesia -> Community-based risk reduction
Low + middle income countries have rising incidence of colorectal cancer (aging population + sedentary lifestyle, westernized behavior lifestyle)
Does westernized behavior necessarily correlate with cancer? And how so? (dangers of the simplified model of civilization = cancer and primitivism = safe from cancer -> How Color Crossed the Cancer Line book)
Cultural influences on health beliefs/values/behaviors
CRC screening less supported in Asia (equipments + specialists costs)
Data collected from observation, interviews, focus group discussions, thematic analysis
Themes:
Food preparation (cook freshly rather than refrigerate)
Food cooking (low sodium salt and limit flavor additives)