The data aggregation problem and health disparities
Third most common cancer in the U.S
Asian American subgroups vary widely -> problem of data registries and research aggregating them into one group
Discussed by Wailoo’s book How Cancer Crossed the Color Line -> historically race and ethnicity has been defined arbitrarily by the dominant group (white) -> all other groups are aggregated in terms because they are ‘other’ to the white group, therefore being blind to each group’s own internal diversity
Heterogeneity in incidence -> related to country of origin, diet, screening, and lifestyle choices
Japanese Americans have the highest incidence, and all incidence are increasing among other groups except for Korean Americans
CRC incidence is highest among non-Hispanic black populations, lowest among Asians/Pacific Islanders
SEER program only started collecting data on Hispanic Americans and Asians/Pacific Islanders since 1990
What does this say about missing data and inability to create historical trends?
Gap between mortality rates among Black and White Americans have increased over the last 3 decades
Disparities exist between races but also within
Screening prevalence lower among ages younger than 65, non-White, less educated, without insurance, recent immigrants, Hispanic people, and those with language barriers
Asians are less likely to screen than non-Hispanic whites
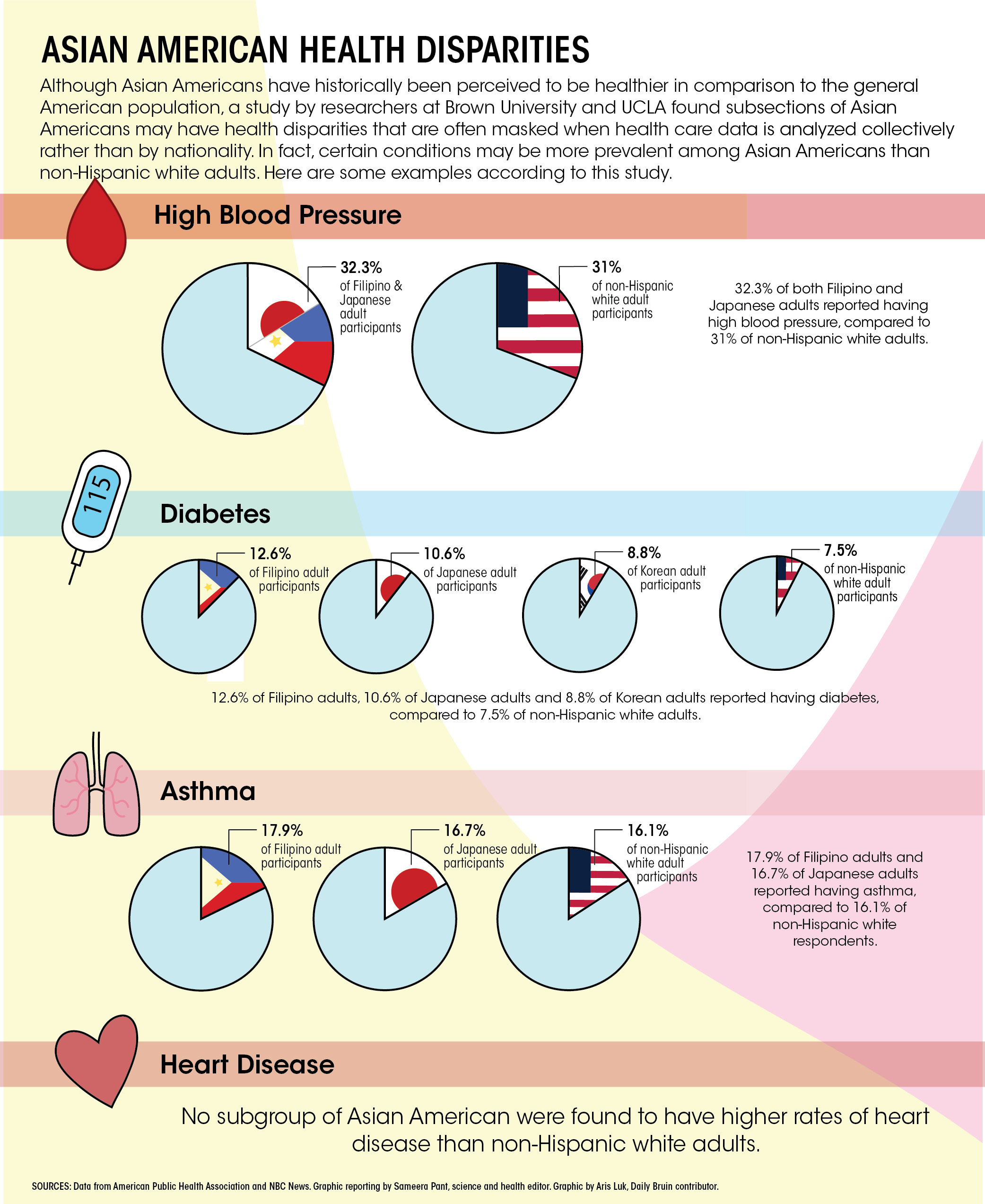
A study finding that data aggregation of Asian American subgroups conceal health risks. Article found from here: https://dailybruin.com/2020/03/06/study-shows-aggregated-data-conceals-asian-american-subgroup-health-problems
A study found “the Western diet increases colon cancer by deregulating bile acid homeostasis, and activating colon cell proliferation”
Dietary chemoprevention -> cultural aspects of diet and lifestyle in Asian Americans in cancer prevention
unpolished Thai rice and reduced CRC risk because of high phytochemical contents
Sea cucumbers, abalones are both Asian delicacies are shown to have anti-tumor properties
Risk factor: Risk increases among Asian Americans as their diet becomes ‘Westernized’
Asians with longer immigration history parallel cancer risk patterns of U.S natives
Asians with more recent immigration history parallel cancer risk patterns of home countries
Reflections/questions
Emphasizes the need for more complete data (Flaws in databases and data collection methods: Primarily in English, did not capture populations with low English proficiency, vary in time frame/sample size/geography, SEER data is more recent on Asians)
Perhaps more data on cultural and behavioral factors that influence prevention and screening?